Rotator Cuff Tears and Rotator Cuff Repair
The rotator cuff consists of four muscles and their tendons. These surround the ball of the shoulder joint.
The muscles fine tune the movements of the shoulder joint and assist other large muscles in moving the arm.
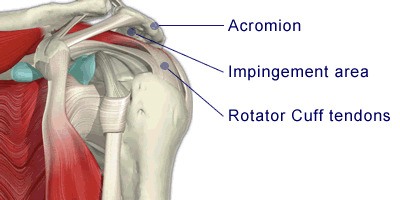
The tendons run under the acromion (the prominent bone at the tip of the shoulder - part of the shoulder blade) where they are very vulnerable to being damaged. This can lead to a tear resulting in a painful, weak shoulder.
The tendon of the rotator cuff passes through a narrow space between the top of the arm bone and a prominent bone on the shoulder blade (the acromion). The tendon is very vulnerable to being pinched here when the arm is moved, especially above the head. Over time this pinching can lead to tears of the tendon; the chance of this increases as we get older.
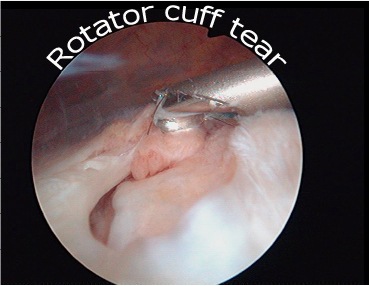
When repeated tearing occurs, the fabric of the tendon becomes weakened and finally, like the cloth at the knees of old trousers, splits. This leads to pain, which can be severe. Weakness of the shoulder can occur, often with clicking and crunching on movement.
Other forms of treatment such as injection and physiotherapy are available, but sometimes it is necessary to repair the tendon. How well this does will depend upon the size of the tear. If we think about the trousers again, the bigger the split in the cloth, the more difficult is the repair and the more likely the repair is to re-tear. Your consultant will have discussed this with you.
The Operation
The operation is done by 'key hole surgery'; usually through three or more 5mm puncture wounds. It involves cutting the coraco-acromial ligament and shaving away part of the acromion bone. This increases the space of the subacromial area and reduces the pressure on the muscle and bursa allowing them to heal.
A repair involves stitching the torn tendon back onto its attachment to the arm bone (Humerus). This is done using tiny anchors with sutures attached to them to reattach the torn tendons back to the bone. The repair should be protected until healing take place (for initial healing - 6 weeks).
Nowadays at the Reading shoulder unit, rarely an open surgery is needed for the repair of torn rotator cuff tendons.
PRP Injection
In recent years, we have been using Platelet Rich Plasma (PRP) to enhance the healing, Platelet Rich Plasma (PRP) is blood plasma with concentrated platelets (the body's repairmen for damaged tissue). The concentrated platelets found in PRP contain growth factors that are vital to initiate and accelerate tissue repair and regeneration. These bioactive proteins initiate connective tissue healing and repair, promote development of new blood vessels, and stimulate the healing process.
What are the Potential Benefits of PRP Treatment?
We have observed that patients that had PRP supplement to their rotator cuff repairs had substantially less pain postoperatively. We believe that the PRP enhances the recovery, we do not have clear scientific evidence for that yet, but there are some case studies that show this.
A major advantage of this treatment is that no foreign substance is used but the patient’s own growth factors from his own blood. There is no risk of any disease transmission.
General Advice
You will usually be in hospital either for a day or overnight. The operation is performed under general anaesthetic and a nerve block in your neck or upper chest that will make your arm 'dead' for 8-12 hours after surgery. This is for post operative pain relief. After this the shoulder may well be sore and you will be given painkillers to help this.
Your arm will remain in a special sling for 6 weeks. This means that you will be unable to use the arm throughout this time and you will be unable to return to work. You will not be allowed to drive for 6-8 weeks after surgery.
A doctor/physiotherapist will see you prior to discharge and you will be taught exercises to do and given further advice to guide you through your recovery.
The length of time that you will be off work will depend on your job but expect a minimum of 6 weeks. For manual workers this may take up to 6 months.
Out patient physiotherapy will be organised for when you leave hospital and may well continue for some considerable time.
You will be guided through the rehabilitation programme by your physiotherapist. It is of the utmost importance that you stick strictly to this programme.
The wounds
This keyhole operation is usually done through three or more 5mm puncture wounds. There may be no stitches only small sticking plaster strips over the wounds. These should be kept dry until healed. This usually takes 5 to 7 days.
Complications
As with all surgery there is a risk of some complications. These are rare, but you should be aware of them before your operation. They include:
- Complications relating to the anaesthetic.
- Infection.
- Injury to the nerves or blood vessels around the shoulder.
- Prolonged stiffness and or pain.
- Failure to achieve successful result.
- A further tear of the tendon. The larger the tear - the more chance there is of this occurring
- Failure to regain strength (dependant upon the size of the tearand the muscle atrophy)
- A need to redo the surgery.
If you require further information please discuss with the doctors either in clinic or on admission.
Guidelines for patients following rotator cuff repair
Introduction
The rotator cuff consists of four muscles and their tendons which surround the ball (humeral head) of the shoulder joint. The muscles fine tune the movements of the shoulder and help keep the ball of the shoulder joint in its socket.
The Operation
This is carried out under a general anaesthetic. The operation is usually performed through the keyhole. However, it is occasionally necessary to make a larger cut over the shoulder. The tendon is repaired by stitching it to the bone. The arm is then placed in a sling to allow for healing.
General guidelines
- Pain: A nerve block is usually used during the surgery. This means that immediately after the operation the shoulder and arm often feel completely numb and weak. This may last for a few hours. After this the shoulder may well be sore and you will be given painkillers to help this whilst in hospital. These can be continued after you are discharged home. Ice packs may also help reduce pain. Wrap crushed ice or frozen peas in a damp, cold cloth and place on the shoulder for up to 15 minutes.
- Wearing a Sling: You will return from theatre wearing a sling. The surgeon/physiotherapist will advise you on how long you are to continue wearing the sling. This is usually for between 3 and 6 weeks depending upon the size of the tear. You will be expected to remove the sling for exercises only. Your physiotherapist will advise you of these.
- The Wound:
Open repair: there is an incision at the top of the shoulder. The stitch is dissolvable but is usually removed at 3 weeks. Keep the wound dry until it is well healed. - Arthroscopic (keyhole) repair: This keyhole operation usually done through two or three 5mm puncture wounds. There will be no stitches; only small sticking plaster strips over the wounds. These should be kept dry until healed. This usually takes 5 to 7 days.
- Driving: You will not be able to drive for a minimum of 8 weeks. Your surgeon will confirm when you may begin.
- Returning to work: This will depend upon the size of your tear and your occupation. You will need to discuss this with your surgeon.
- Leisure activities: This will depend upon the size of the tear. Your physiotherapist and surgeon will advise you when it is safe to resume your leisure activities.
- Follow up appointments: An appointment will be made for you to see a physiotherapist after your discharge and you will be seen at The Shoulder Unit at 3 weeks. You will be monitored by a physiotherapist throughout your rehabilitation
- Exercises: You may well be expected to perform the following exercises. Your physiotherapist will teach you the following exercises before you leave hospital, if appropriate:
- With your arm in the sling move your hand up and down at the wrist.
- With your arm out of the sling bend and straighten the elbow
- With your arm in the sling and the elbow bent at your side, turn the hand to face the ceiling and then the ground.
Repeat these exercises four times per day. The number you should perform at each session will be recorded for you by your physiotherapist.
Continue these exercises until otherwise advised by your physiotherapist.
If your wound changes in appearance, weeps fluid or pus or you feel unwell with a high temperature, contact your GP.
If you have a query concerning your exercises contact the physiotherapy department where you are receiving treatment.