Biceps Tendo Lesions / SLAP tears
Print PdfBiceps tendon disorders SLAP (Superior labrum) Tears
Biceps tendon disorders / SLAP (Superior labrum) tears
Introduction
The shoulder is a ball and socket joint. The socket of the shoulder is like a flat saucer, while the ball is a hemisphere. This arrangement of a shallow socket and a hemispherical ball allows for a large range of movement, but makes the joint prone to instability. To increase the stability of the joint without compromising the movement, the socket is deepened by the attachment of a cartilagenous labrum along its circumference called the 'Labrum' which resembles a ring of gristle around the socket.
Along the upper part of this ring, the tendon of the biceps attaches to the labrum (Fig 1).
Biceps Tendinosis & Tear of the Long head of Biceps (LHB)
Shoulder pain and dysfunction can arise as a result of long head of the biceps (LHB) pathologies, which broadly speaking can be divided into degenerative, inflammatory, instability, entrapment, and traumatic and sport-related types.
Often, there may occur spontanous rupture of the long head of the biceps (LHB), appearing as a"lump" in the front of the lower arm. It is named "Popeye" sign (after Popeye the sailor...). It is usually accompanies rotator cuff tear and rarely isolated LHB tear.
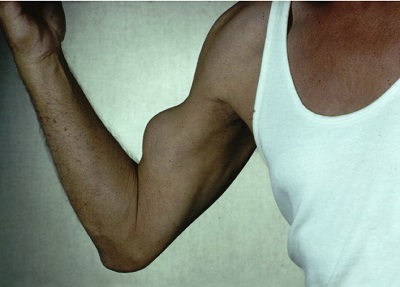
Rupture of the long head of the biceps (LHB) with "Popeye" sign
Spontanous rupture of the long head of the biceps (LHB) usually doesn't require any specific treatment and doesn't lead to any functional deficit.
Operative management for LHB disorders
Operative management for LHB disorders includes synovectomy, tendon debridement, transfer, repair of partial tears, and reconstruction of the damaged pulley (for LHB instability); however, tenotomy (cutting the tendon) and tenodesis (fixing the tendon to the humeral head) are by far the most common surgical choices.

There is still debate among shoulder surgeons: Tenotomy or Tenodesis?
Surgical options for symptomatic pathologies of the long head of the biceps (LHB) include tenotomy (cutting the tendon) and tenodesis (fixing the tendon to the humeral head).
Tenotomy (cutting the tendon) is surgically simple and quick, does not require immobilization, and avoids implant complications. However, it may be associated with residual “Popeye” muscle deformity and biceps muscle cramps.
Tenodesis avoids "Popeye" deformity, but it is technically a more difficult operation with a longer rehabilitation period and possible implant complications.
Other than the increased risk of the "Popeye" deformity and mucle cramps with tenotomy, Both procedures have similar rates of success with comparable outcome scores and rates of satisfaction.
We have described a novel technique for arthroscopic LHB tenotomy/tenodesis that avoids the classic "Popeye" muscle deformity and the risk of muscle cramps. We named it the “Anchor Shape” technique or "the Brazilian" technique - acknoledgement to Dr. Arildo Eustáquio Paim of Belo Horizonte, Brazil, from whom we learned this technique.

What is a SLAP lesion?
A SLAP lesion occurs when the upper labrum (superior labrum) is torn at or near it's attachment with the biceps. The tear occurs on either side of the 12 o'clock position on a clock face and hence the name Superior Labrum Anterior and Posterior (SLAP) Tear.
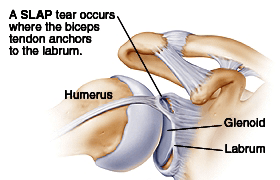
Fig 1: Diagramatic representation of the labrum & a SLAP lesion
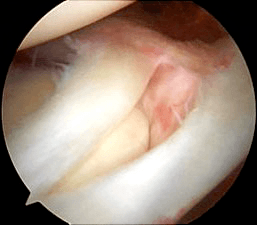
Fig 2: SLAP Lesion at arthroscopy
How does it occur?
A SLAP tear usually occurs with heavy forceful lifting, repeated overhead activity (tennis, throwing) or a fall on the outstretched hand.
How is it Diagnosed?
The diagnosis is made from the history and findings at examination. The patient can present with pain or mechanical symptoms in the joint. If associated with an anterior labral tear, they may present with a history of shoulder instability or dislocations. In addition, special tests such as an MR-Arthrogram help in confirming the diagnosis. However, in the abscence of findings on examination or MR, a diagnostic arthroscopy may sometimes be performed.
How is it treated?
If symptomatic, the tear can be treated surgically using 'key hole' surgical technique. The procedure is done as a day surgical procedure. Using special bone anchors (screws) and sutures, the torn labrum is attached back to its normal position. Sometimes, the tear may be irreparable. In such cases, it is smoothed down (debrided) to a stable surface (Tenodesis).
General Advice
You will usually be in hospital either for a day or overnight. A doctor/physiotherapist will see you prior to discharge and you will be taught exercises to do and given further advice to guide you through your recovery. You will be given a sling. This is provided for upto 6 weeks. You should avoid forced straightening of the elbow or heavy lifting for atleast 6 weeks. You can expect to be back at work between 8-10 weeks depending on your job. Your symptoms should be approximately 80% better after three months but may take 6 months to totally settle.
Complications
As with all surgery there is a risk of some complications. These are rare, but you should be aware of them before your operation. They include:
- Complications relating to the anaesthetic.
- Infection.
- Failure to achieve successful result.
- A need to redo the surgery.
- Injury to the nerves or blood vessels around the shoulder.
- fracture
- Implant failure
- Complete tear of Biceps.
- Prolonged stiffness and or pain.
If you require further information please discuss with the doctors either in clinic or on admission.
What to expect about the operation and rehabilitation
- Pain: A supplementary local anaesthetic or nerve block is used during the operation which means that immediately after the operation the shoulder and arm may feel numb. This may last a few hours. After this the shoulder may well be sore and you will be given painkillers to help this whilst in hospital. These can be continued after you are discharged home. Ice packs may also help reduce pain. Wrap frozen peas or crushed ice in a damp, cold cloth and place on the shoulder for up to 15 minutes.
- Wearing a Sling: You will return from theatre wearing a sling. This is required for upto 6 weeks, to allow the repair to heal. You should avoid forced straightening of the elbow or heavy lifting for at least 6 weeks.
- The Wound: This is a keyhole operation usually done through three to five 4mm puncture wounds. There will be no stitches only small sticking plaster strips over the wounds. These should be kept dry until healed. This usually takes 5 to 7 days.
- Driving: You may begin driving 6 weeks after your operation.
- Returning to work: This will depend on your occupation. If you are in a sedentary job you may return as soon as you feel able usually after one week. If your job involves heavy lifting or using your arm above shoulder height you may require a longer period of absence (8 weeks).
- Leisure activities: You should avoid sustained, repetitive overhead activities or activities involving forced elbow extension for three months. Golf can begin at 12 weeks. For guidance on DIY and racquet sports you should speak with your physiotherapist.
- Follow up Appointment: You will be made a follow up appointment at the Shoulder Unit for around three weeks after your surgery. At this stage you will be reviewed by the specialist physiotherapist or Consultant who will check your progress, make sure you are moving your arm, and give you further exercises as appropriate.
- Exercises: After leaving hospital you should exercise the arm frequently throughout the day. The arm may feel sore whilst you are doing the exercises but there should be no intense or lasting pain. Aim for four exercise sessions per day. The physiotherapist will advise you regarding the exercises prior to discharge.
If your wound changes in appearance, weeps fluid or pus or you feel unwell with a high temperature, contact your GP.
If you have a query concerning your exercises contact the physiotherapy department where you are receiving treatment.