AC Joint Dislocation & Reconstruction
Guidelines for patients following Modified Weaver-Dunn procedure for Reconstruction of the Acromioclavicular joint
Infinity loop Brochure
Introduction
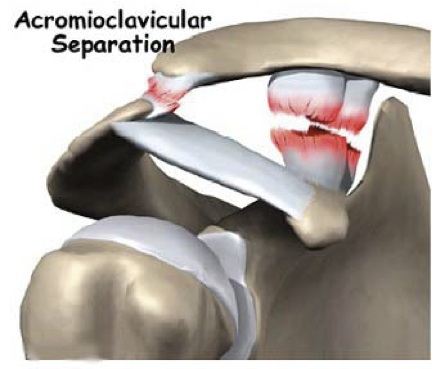
The Acromioclavicular joint (ACJ) is part of the shoulder complex. It is situated on top of the shoulder joining the clavicle (collar bone) to the scapular (shoulder blade).The joint can be separated (dislocated) as a result of injury. Ligaments are torn and in severe cases surgery is required to stablise the joint.
The operation
The procedure involves reconstruction of the AC Joint ligaments: both the Coraco-Clavicular (CC) ligaments and the Acromio-Clavicular (AC) ligaments, utilising artificial ligament as a scaffold to reconstruct and stabilise the joint. This reconstruction is supported by an absorbable cord. We use as well PRP - platelet Rich Plasma, made from the patient’s own blood and contain a high concentration of platelets with all the growth factors, in order to enhance the healing.
The operation can be performed using mini-open surgery through small 5cm incision over the top-front of the shoulder.
Complications
As with all surgery there is a risk of some complications. These are rare, but you should be aware of them before your operation.
They include:
- Complications relating to the anaesthetic.
- Infection.
- Failure to achieve successful result.
- A need to redo the surgery.
- Injury to the nerves or blood vessels around the shoulder.
- fracture
- Prolonged stiffness and or pain.
- Implant failure
- Re-tear of the ligaments.
If you require further information please discuss with the doctors either in clinic or on admission.
You will usually be in hospital either for a day or overnight. A doctor/physiotherapist will see you prior to discharge and you will be taught exercises to do and given further advice to guide you through your recovery.
GENERAL GUIDELINES
- Pain: A nerve block may be used during the procedure, which means that immediately after the operation the shoulder and arm can feel numb for a few hours. The shoulder will be sore when this wears off and this may last for the first few weeks. It is important that you continue to take the painkillers. Ice packs may also help reduce pain. Wrap frozen peas/crushed ice in a damp, cold towel and place on the shoulder for up to 15 minutes.
- Wearing a sling: You will return from theatre wearing a sling with a body belt. It should be worn under your clothes for three weeks. Only very gentle movements will be allowed under the guidelines of your physiotherapist i.e. for hygiene. After three weeks the body belt will be removed and you will continue to wear the sling over the clothes for a further three weeks. At this time you will start formal physiotherapy.
- The wound:
Open repair: there is an incision of 5cms over the top of the shoulder. The stitch is dissolvable but may require trimming at 3 weeks. Keep the wound dry until it is well healed. - If your wound changes in appearance, weeps fluid, pus, or you feel unwell with a high temperature, contact immediately your GP.
- Posture: Before starting any activity/exercise it is important to position your shoulders correctly. This allows normal shoulder function. Gently move your shoulder blades down and in towards the spine but not in a braced back position.
- Driving You will not be able to drive for a minimum of 8 weeks. Your surgeon will confirm when you may begin.
- Returning to work: This will depend upon your occupation. You will need to discuss this with your surgeon. Remember you will be completely one-handed for the first 6 weeks and all movements or activities above shoulder level should be avoided for at least 12 weeks from your operation.
- Leisure activities: Your physiotherapist and surgeon will advise you when it is safe to resume your leisure activities.
- Follow up appointments: You will be asked to make an appointment to be reviewed at The Shoulder Unit approximately three weeks after your procedure. You will be reviewed by your surgeon/specialist physiotherapist who will check your progress.
- Progression: This is variable. Following discharge your pain will slowly decrease and you will become more confident. After 6 weeks your physiotherapist will guide you through an appropriate exercise programme to help you regain full function.
- Exercises: You will perform only elbow, wrist and hand exercises for the first 3 weeks.Your physiotherapist will teach you the following excursuses.
- Keep your arm in the sling and move your hand up and down at the wrist.
- With your arm in the sling and the elbow bent at your side, turn the hand to face the ceiling and then the ground.
- With arm in the sling regularly shrug shoulders up and down and circle forwards and backwards
- In sitting, take your arm out of the sling, bend and straighten the elbow on to your lap.
Repeat each exercise 10 times hourly. Continue these exercises until otherwise advised by your physiotherapist.