Impingement Syndrome / Acromioclavicular Joint (AC Joint) Arthritis
Arthroscopic Subacromial Decompression/ Acromioclavicular Joint Excision Arthroplasty
Introduction
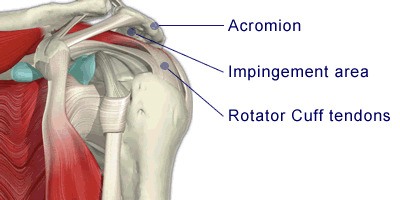
The subacromial area lies between the top of the arm bone (humerus) and a bony prominence on the shoulder blade (acromion). The coracoacromial ligament completes the arch.
A muscle and fluid filled cushion (bursa) lie between the arm bone and acromion. With certain movements and positions these structures can become pinched and inflamed. The pain that you have been experiencing is caused by this pinching and is typically felt on movements such as reaching and putting your arm into a jacket sleeve.
The Acromio-clavicular Joint (ACJ) is a small joint formed between the summit of the shoulder blade (acromion) and the collar-bone (clavicle).This joint can be a frequent source of pain in the shoulder region, especially while performing movements at or above the level of the shoulder. Moving ones arm across the chest at shoulder level, to touch the opposite shoulder can produce significant discomfort if this joint is affected.
Sometimes a calcific deposit (Calcifying tendonitis) is found in the tendons and this may be the cause of the symptoms.
The Operation
The operation is done by 'key hole surgery'; usually through two or three 5mm puncture wounds. It involves cutting the ligament and shaving away part of the acromion bone. This increases the space of the subacromial area and reduces the pressure on the muscle and bursa allowing them to heal.
The operation aims to increase the size of the subacromial area and reduce the pressure on the muscle. It involves cutting the coraco-acromial ligament and shaving away part of the acromion bone (ASD). This allows the muscle to heal.
Pain may arise as well from the small joint between the shoulder blade and the collar bone (Acromio-clavicular joint (AC joint)) due to a cartilage tear or arthritis with wear & tear. In these cases resection arthroplasty of the AC joint with removal of few milimeters of bone from each side of this joint is performed.
If a calcific deposit will be found in the tendons, this will be excised to allow the tendons to heal.
Your shoulder will be examined under anaesthetic (EUA), if it will be found stiff with restricted movement - manipulation under anaesthetic (MUA) for release of the contracture may be needed.
If a rotator cuff tear is detected during arthroscopy, the surgeon may need to repair this torn tendon*.
A repair involves stitching the torn tendon back onto its attachment to the arm bone (Humerus). This is done using tiny anchors with sutures attached to them to reattach the torn tendons back to the bone. The repair should be protected until healing takes place (for initial healing - 6 weeks).
*This will involve a different post operative regime to ASD - you will NOT BE ALLOWED to use your arm or drive for 6-8 weeks.
If you wish that the torn tendon will NOT be repaired - please let the surgeon know before surgery!
General Advice
You will usually be in hospital either for a day or overnight. A doctor/physiotherapist will see you prior to discharge and you will be taught exercises to do and given further advice to guide you through your recovery. You will be given a sling. This is provided purely to keep your arm comfortable. It may be taken off as much as you wish and discarded as soon as possible. You will be encouraged to use your arm. You should be back at work between one and four weeks depending on your job. Your symptoms should be approximately 80% better after three months but may take a year to totally settle.
Complications
As with all surgery there is a risk of some complications. These are rare, but you should be aware of them before your operation.
They include:
- Complications relating to the anaesthetic.
- Infection.
- Failure to achieve successful result.
- A need to redo the surgery.
- Injury to the nerves or blood vessels around the shoulder.
- fracture
- Prolonged stiffness and or pain.
If you require further information please discuss with the doctors either in clinic or on admission.
What to expect about the operation and rehabilitation
- Pain: A supplementary local anaesthetic or nerve block is used during the operation which means that immediately after the operation the shoulder and arm may feel numb. This may last a few hours. After this the shoulder may well be sore and you will be given painkillers to help this whilst in hospital. These can be continued after you are discharged home. Ice packs may also help reduce pain. Wrap frozen peas or crushed ice in a damp, cold cloth and place on the shoulder for up to 15 minutes.
- Wearing a Sling: You will return from theatre wearing a sling. This is for comfort only and should be discarded as soon as possible (usually within the first 1 to 2 days). Some people find it helpful to continue to wear the sling at night for a little longer if the shoulder feels sore. (Please note - If a rotator cuff tear is found and repaired, the sling may be required for 6-8 weeks.)
- The Wound: This is a keyhole operation usually done through two or three 5mm puncture wounds. There will be no stitches only small sticking plaster strips over the wounds. These should be kept dry until healed. This usually takes 5 to 7 days.
- Driving: You may begin driving one week after your operation or when you feel comfortable.
- Returning to work: This will depend on your occupation. If you are in a sedentary job you may return as soon as you feel able usually after one week. If your job involves heavy lifting or using your arm above shoulder height you may require a longer period of absence.
- Leisure activities: You should avoid sustained, repetitive overhead activities for three months. With regard to swimming you may begin breaststroke as soon as you are comfortable but you should wait three months before resuming front crawl. Golf can begin at six weeks. For guidance on DIY and racquet sports you should speak with your physiotherapist
- Follow up Appointment: You will be made a follow up appointment at the Shoulder Unit for around three weeks after your surgery. At this stage you will be reviewed by the specialist physiotherapist or Consultant who will check your progress, make sure you are moving your arm, and give you further exercises as appropriate.
- Progression: This is variable. However experience shows us that by 3 weeks movement below shoulder height becomes more comfortable. By this stage you should have almost full range of movement although there will probably be discomfort when moving the arm above the head. At three months after your surgery your symptoms should be approximately 80% better and you will continue to improve for up to a year following the procedure.
- Exercises: After leaving hospital you should exercise the arm frequently throughout the day. The arm may feel sore whilst you are doing the exercises but there should be no intense or lasting pain. Aim for four exercise sessions per day.
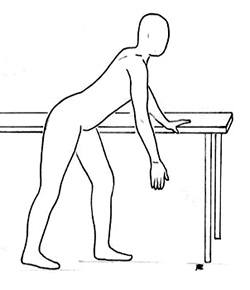
- 1) Stand. Lean forwards. Let your arm hang down. Swing your arm forwards and backwards. Repeat 10 times. (Shown for the right shoulder).
- 2) Stand. Lean forwards.
Let your arm hang down.
Circle your arm clockwise & anti-clockwise.
Repeat 10 times.
(Shown for right shoulder). 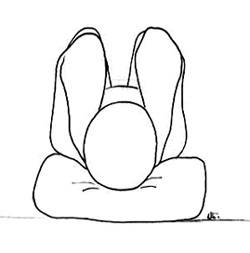
- 3) Lying or sitting. Put your hands behind your head, and gently stretch the elbows towards the floor/ backwards to feel a gentle stretch on the front of your shoulders. Repeat 5 times.
- 4) Lying on your back. Support your operated arm with the other arm and lift it up overhead. Repeat 10 times. (Shown for right shoulder).

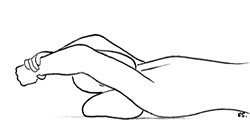
- 5) Lying on your back. Grasp a stick in both your hands. Lift the stick up and gently take overhead until you feel a gentle stretch in your shoulder. Repeat 10 times.

- 6) Take your affected arm across your body to rest the hand on the opposite shoulder. Grasp the elbow with your good hand and gently stretch the arm across your body. Repeat 5 times.

- 7) Lying on your back, keeping the elbow to your side. Hold a stick in your hands. Move the stick sideways, gently pushing the hand on your operated arm outwards. Repeat 5 times.
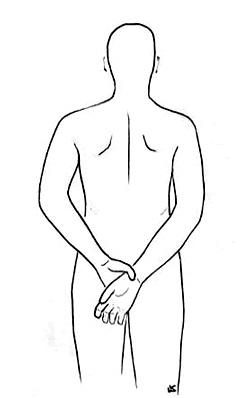
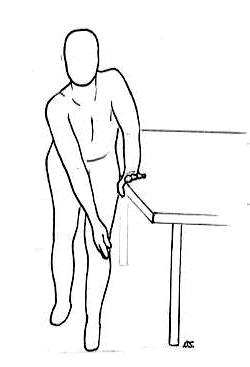
- 8) Standing with your arms behind your back. Grasp the wrist of your operated arm and gently stretch the hand on your affected arm towards the opposite buttock. Then slide your hands up your back. Repeat 5 times.
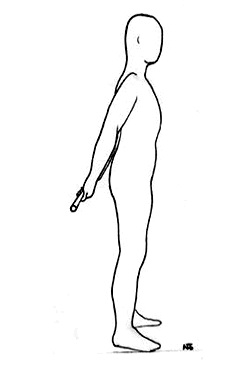
- 9) Standing with a your arms behind your back and grasp a stick between them. Gently lift the stick up away from your body. Repeat 5 times.
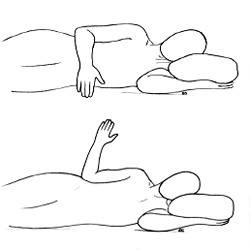
- 10) Lying on side, with operated arm upwards. Keep the elbow bent and close to your side. Lift the hand up away from your body. Repeat 10 times.
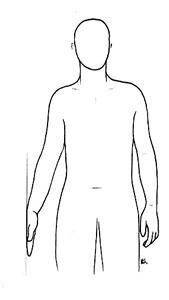
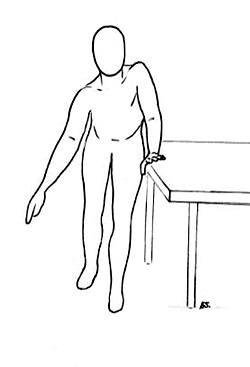
- 11) Stand sideways with operated arm against a wall. Keep the arm close to your side, and push the hand against the wall, hold for 5 seconds. Repeat 10 times.
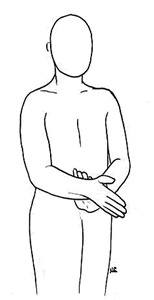
- 12) Standing, with elbow flexed to 90 degrees, and held close to body, grasp the wrist of the affected arm with the good hand. Attempt to move the hand of the affected arm inward resisting the motion with the good hand. Keep the affected arm still. Hold for 5 seconds. Repeat 10 times.

- 13) Standing, with elbow flexed to 90 degrees, and held close to body, grasp the wrist of the affected arm with the good hand. Attempt to move the hand of the affected arm outward resisting the motion with the good hand. Keep the affected arm still. Hold 5 seconds. Repeat 10 times.